 Skip to content
Skip to content 
Last Updated on August 13, 2025 by John Hookway
You might notice your child or someone else acting in a new way and wonder if it could be autism. This is an important question that deserves attention.
Many parents in the United States do not receive clear answers early on. For example, only about 30% of parents with kids ages 9 to 35 months complete developmental questionnaires. Just over half of children with autism receive Autism Screenings by age three, as shown in the table below.
| Measure | Percentage |
|---|---|
| Parents of children 9-35 months asked to fill out questionnaire | ~30% |
| Children 9-35 months receiving developmental surveillance | ~37% |
| Children aged 8 years with ASD evaluated by 36 months | 50.3% |
| Children aged 8 years with first evaluation by age 3 years | 42-43% |
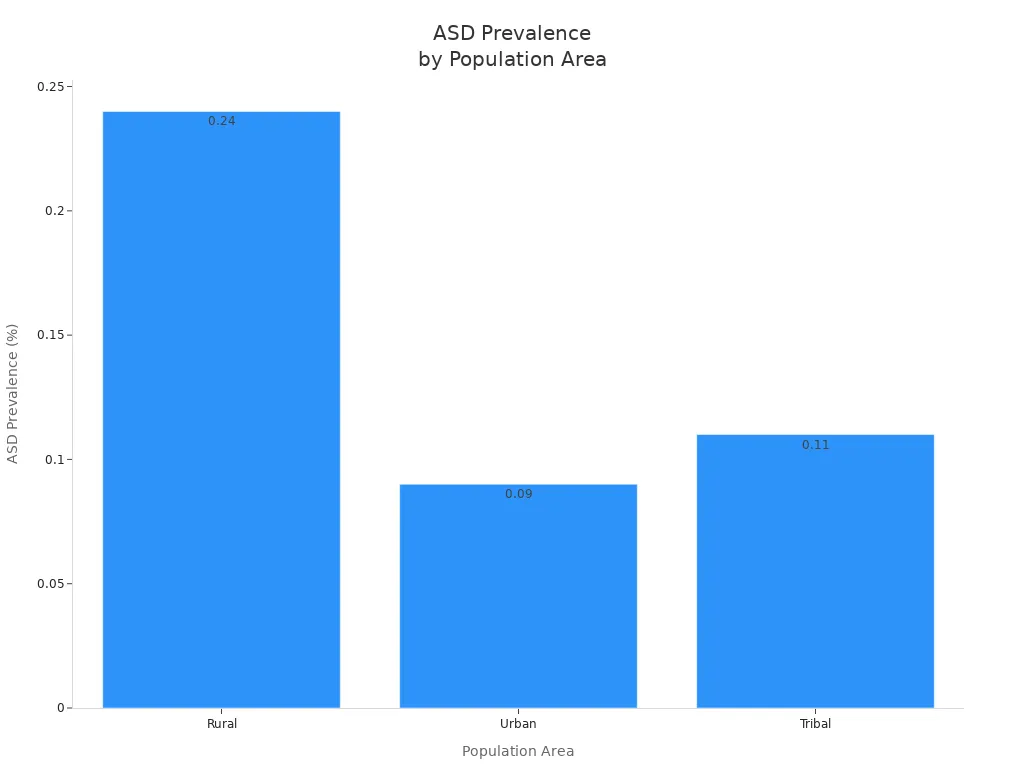
Screening rates vary by location. In rural areas, children may face more challenges getting timely Autism Screenings. Autism is diagnosed more frequently in these areas compared to cities.
You deserve answers that help you understand what is happening. These answers can guide your next steps. Early Autism Screenings can make a significant difference.
Key Takeaways
- Early autism screenings find signs sooner. This helps kids get diagnosed faster. It also means they get help sooner.
- Screenings link families to therapies and resources. These things help a child grow and do better each day.
- The screening process uses questionnaires, observations, and expert checks. These happen over a few visits.
- Early diagnosis lowers stress for families. It helps them make smart plans for their child’s care.
- Working with doctors and support groups after screening helps a lot. It leads to better results and more confidence.
Clarity from Screenings
Autism Screenings help you learn about your child’s growth. These tests give answers when you see different behaviors. You might feel worried or confused, but screenings can help you understand.
- Early Autism Screenings at checkups help you get a referral if needed.
- When you know what is going on, you feel less stress. You can focus on helping your child.
- Screening results connect you to resources and support groups for your family.
- Early identification lets your child start therapies sooner. These include speech therapy, occupational therapy, and behavioral programs.
- Doctors and scientists say early detection leads to better treatment plans. This is important during key growth times.
- Early diagnosis helps stop other problems by treating symptoms fast.
- You gain confidence and feel more in control. This helps you support your child at home and school.
- Researchers keep making screening tools better and more helpful.
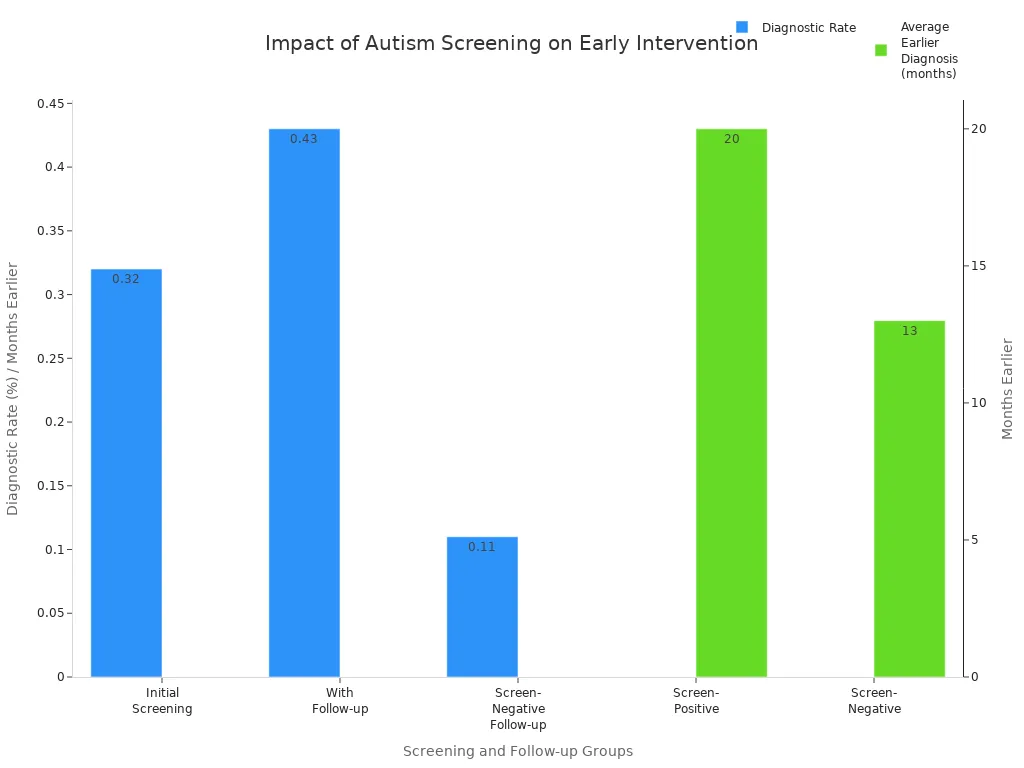
The chart below shows how early screenings help. Kids who get screened at 18 and 24 months are diagnosed about 20 months earlier.
Early diagnosis means they get help sooner. This improves their long-term outcomes.
Next Steps After Screening
After an Autism Screening, you may wonder what comes next. The results help you decide your next steps and find support.
People diagnosed later in life often have more problems. They miss out on resources and support. One adult with ASD said life is still hard, even with a diagnosis and help. The world is not made for them. This shows why early diagnosis and better support are needed.
The study says early diagnosis helps people and families get support. This makes life better. Late diagnosis can cause regret and missed chances for help.
Most families get a clear plan after screening. You may get a referral for a full assessment. If your child is diagnosed, you can get therapies and support.
These may include:
- Communication and relationship-building therapies
- Emotional regulation support
- Cognitive Behavioral Therapy (CBT) for anxiety, depression, and sleep problems
- Medications for symptoms like anxiety, aggression, or hyperactivity
- Nutritional supplements, such as omega-3 fatty acids, for irritability
Outcomes after screening are different for each child. Some kids become more independent. Others need support for life. Many make steady progress with the right help. The table below shows the most common outcomes:
| Outcome Trajectory | Description | Estimated Proportion |
|---|---|---|
| Optimal Outcome | Diagnosed in childhood, become independent, and have fewer autism symptoms. Core features stay but do not cause big problems. | ~20% |
| Lifelong Support Needed | Need a lot of support all the time, often with other disabilities. Progress is slow but important. | ~20% |
| Middle Trajectory | Most kids make slow but steady progress. They keep getting help from the community and therapy. Autism features stay. | ~60% |
You may face some barriers along the way. These can be high costs, not enough trained professionals, or few resources nearby.
Some families feel unsure or have trouble talking to doctors. Knowing these problems helps you get ready and find help.
Autism Screenings give you a place to start. They help you know what is happening and what to do next. With early answers, you can make good choices and help your child grow.
Autism Screenings Explained
Screening Tools
You might wonder what tools doctors use for Autism Screenings. These tools help find early signs of autism. They also help decide what to do next for your child. Most tools collect information from you and watch how your child acts.
- The Modified Checklist for Autism in Toddlers (M-CHAT™) is a set of questions for parents. You answer questions about your child’s social and talking skills.
- The Screening Tool for Autism in Toddlers and Young Children (STAT™) uses short games and tasks. It checks how your child plays, copies others, and talks. It takes about 20 minutes to finish.
- General developmental screening tools, like the Ages and Stages Questionnaires (ASQ®), look at many parts of growth. You fill these out based on your child’s age.
- The Communication and Symbolic Behavior Scales (CSBS DP™) and Parents’ Evaluation of Developmental Status (PEDS Tools®) also use parent answers to check for delays.
Autism Screenings use these tools to look for signs of autism. They do not give a final diagnosis. If the results show concerns, your doctor may suggest a full checkup.
Specialists may also talk with you and watch your child. For example, the Autism Diagnostic Observation Schedule (ADOS-2) lets a trained person watch your child’s social and talking skills in a set way.
What Is Assessed
Autism Screenings check how your child acts, talks, and plays. Doctors look for certain skills and behaviors at each age. The table below shows some important things they check:
| Age Milestone | Behaviors and Developmental Milestones Assessed |
|---|---|
| By 4 months | Smiling, cooing, bringing hands to mouth |
| By 6 months | Playing with others, looking in mirror, sitting without support |
| By 9 months | Making sounds, understanding “no”, crawling |
| By 1 year | Playing peekaboo, following directions |
| By 18 months | Speaking words, eating with spoon, walking |
| By 2 years | Noticing emotions, using two-word phrases |
| By 3 years | Naming pictures, dressing, running easily |
During Autism Screenings, you answer questions about your child’s eye contact, how they react to their name, speech, gestures, and repeated movements.
Doctors also look for special patterns in social skills and play. These checks help tell autism apart from other problems. If your child shows signs, the screening helps you move to the next step—a full checkup.
Screening Process
What to Expect
When you start Autism Screenings, you go through several steps. First, you or your doctor notice signs and decide to get help. You might call a clinic or get a referral.
Next, you collect information about your child’s growth and any odd behaviors. You fill out forms and share records from school or other places.
Here is how the screening process usually goes:
- Talk to your doctor about your worries and ask for a referral.
- Fill out forms about your child’s growth and actions.
- Wait for a full checkup if needed.
- Go to an in-person visit. This can include interviews, games, and watching your child.
- Meet with experts like psychologists, pediatricians, and speech therapists.
- Get a full report with results and advice.
The process takes more than one visit. The first phone call lasts 15 to 30 minutes. Filling out forms takes 30 to 60 minutes.
In-person visits last 2 to 4 hours and may happen over a few days. Parent interviews take 1 to 2 hours. The whole process usually takes 1 to 4 weeks, depending on schedules.
Early Autism Screenings help kids get answers faster. Adults can also use this process to learn more.
After the Screening
After screening, you get a detailed report. The team talks with you about the results and answers your questions.
If the screening shows signs of autism, you may get a referral for more tests. This next step can include more interviews, medical checks, and visits with experts.
You may get advice for early help or special education. The team explains what to do next and gives you resources.
You can start therapy or support right away if needed. The report may take a few weeks, but you can plan care as soon as you get results.
| Step | Duration | Notes |
|---|---|---|
| Initial phone intake | 15–30 minutes | Share worries and basic details |
| Questionnaires and forms | 30–60 minutes | Finish before your first visit |
| In-person assessment | 2–4 hours | May be split into a few sessions |
| Parent interviews | 1–2 hours | Talk about your child’s history |
| Follow-up feedback session | About 1 hour | Go over results and next steps |
Autism Screenings help you know what to do next. You get answers, support, and a plan to help your child or yourself do well.
Benefits and Concerns
Understanding and Support
Getting early autism screening helps your child in many ways. Early diagnosis gives you answers. It can lower your worry.
You can make better plans for your child. Kids who get help early do better in speech and learning. They also get better at talking and making friends. This helps them do well in school and daily life.
- Early diagnosis gives families clear answers and less stress.
- Kids get special therapies during important growth times.
- Studies show early help boosts IQ, speech, and school skills.
- Finding out early lets you pick the best treatments.
- Early help can save money for families and the community.
You also get support from many places. Therapies like speech, occupational, and behavioral therapy are available. You can join support groups and workshops to learn how to help your child at home.
Community groups give you emotional support and ways to handle stress. Insurance and government programs help with costs. Good relationships with teachers and therapists help make better school plans.
Early screening connects you to resources and other families. You learn to face challenges and celebrate progress together.
Addressing Misconceptions
There are many myths about autism screening. Some people think one test can diagnose autism, but it takes more than one test. Specialists need to do several checks. Autism happens in both boys and girls.
Girls may show different signs. Some people think kids will outgrow autism, but it lasts for life. Early help makes skills and life better.
You might worry about wrong results. Sometimes, behaviors look like autism but are not. Experts use careful checks to avoid mistakes. They suggest getting another opinion if you are still unsure. Screening tools work best when used more than once and with parent input.
| Myth | Fact |
|---|---|
| One test diagnoses autism | Diagnosis needs multiple assessments and specialists |
| Only boys get autism | Autism affects boys and girls, but girls may be underdiagnosed |
| Children outgrow autism | Autism is lifelong, but early help improves outcomes |
You help get the right diagnosis by sharing your worries and your child’s history. Working together with professionals leads to better support and long-term success.
Autism Screenings help you find out if it is autism. They give you clear facts and show what to do next. Early screening helps you get a diagnosis faster. It also helps you get support services sooner. You can:
- Get care and follow-up quickly.
- Get past problems with treatment, even in places with less help.
- Use telemedicine to find answers and get support early.
Groups like the CDC, American Academy of Pediatrics, and Autism Society say Autism Screenings are important first steps. If you worry about your child, you should:
- Set up a full checkup with a trained provider.
- Join support groups and learn about different therapies.
- Work with your child’s school to make a support plan.
Acting early helps you get answers and support for your family.
FAQ
What is the difference between autism screening and diagnosis?
Screening checks for early signs of autism. Diagnosis confirms if someone has autism after more tests. You start with screening. If results show concerns, you move to a full evaluation.
What happens if my child does not pass the autism screening?
If your child does not pass, you get a referral for a full assessment. This helps experts learn more about your child’s needs. You can start support and therapies early.
What should I bring to an autism screening appointment?
Bring your child’s medical records, school reports, and any notes about behaviors you have seen. You may also bring completed questionnaires. This information helps the team understand your child better.
What resources can help after an autism screening?
You can find help from local support groups, therapy centers, and online communities. Doctors may suggest speech or occupational therapy. Many families use resources from the CDC or Autism Society.





